Define the goals of your data collection session.
What do you want to find out? These goals should be based on your project goals.
1. Conducting a survey or interviews to identify the key factors that are important to people when choosing a health insurance company, and how ePA policies and practices fit into those factors.
2. Based on the insights from the survey or interviews, designing a set of questions that would help users compare different health insurance companies and make an informed decision. These questions could cover aspects such as the availability and accessibility of electronic patient records, data privacy and security policies, and the quality and accessibility of healthcare services.
3. Creating a digital tool or application (Wahl-O-Mat) that presents the user with a set of questions based on their preferences and priorities, and provides them with a recommendation on which health insurance company to choose.
4. Testing the effectiveness of the tool by dividing users into two groups – one group uses the tool to choose a health insurance company, while the other group relies on Google or other search engines to find information. You could then compare the outcomes between the two groups to determine the efficacy of the tool in helping people make an informed decision.
Based on your goal, derive the stakeholders you want to collect data from.
What are your stakeholders? Whom do you need to approach (i.e., who is indispensable for your achieving project goals)?
- health insurance companies
- people that are looking for a new health insurance company
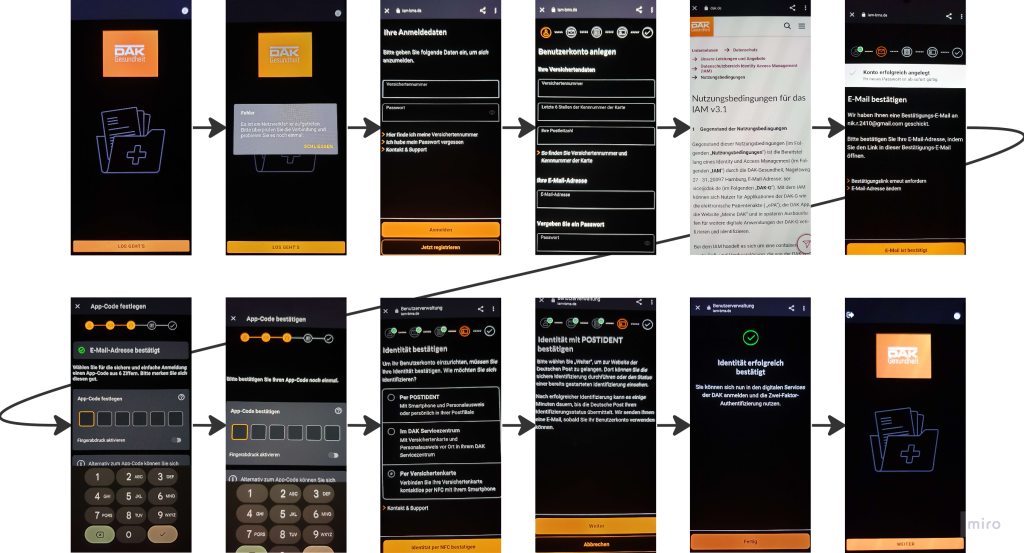
Start with collecting information without approaching your stakeholders (so-called secondary data collection). Use existing websites, app information, and experience the app by yourself. Describe the app you are using in detail (who has developed the app, why, what functionality is available, how can people access the app, etc.)
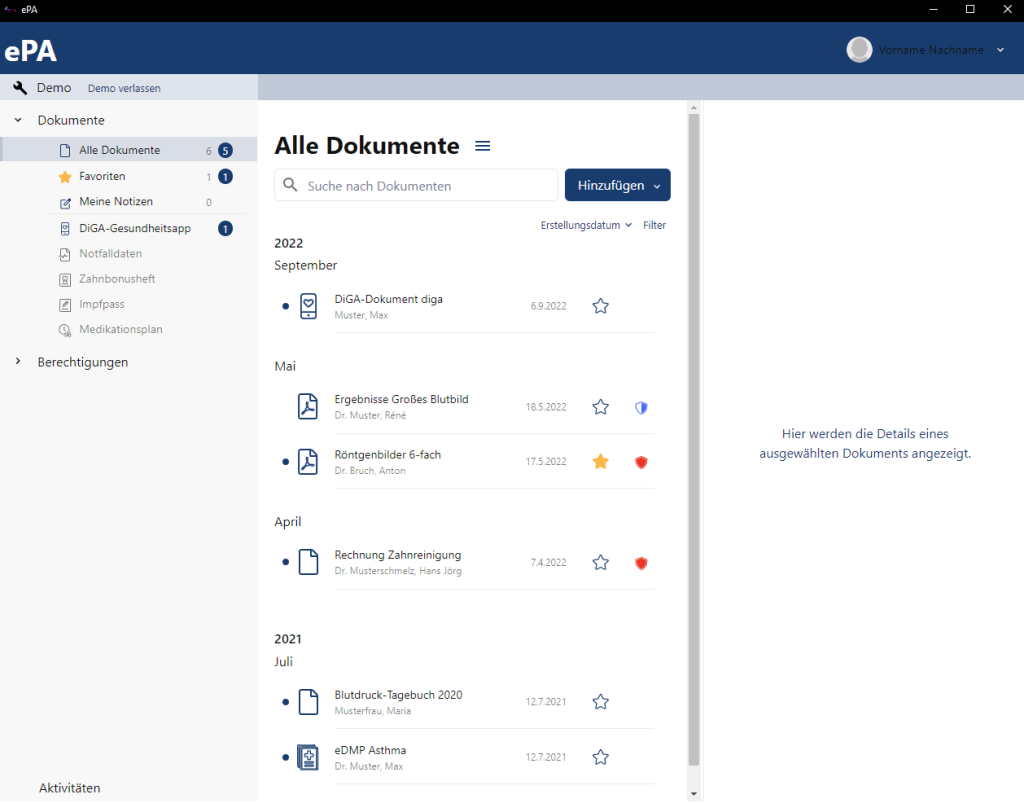
The ePA is a digital health record app developed by the Gematik, a German government organization responsible for the digitalization of the healthcare system. The ePA app is designed to provide users with a secure and centralized platform to manage their health records and interact with healthcare providers.
The app is available to all insured persons in the German health insurance system and can be downloaded for free from the app store on Android or iOS devices from the health insurance company. Once downloaded you can sign in using the approach given by the health insurance company.
The ePA app offers a range of functionalities, including the ability to view and manage personal health records, such as medical reports, vaccination records, and medication plans. The app also enables users to share their health records with healthcare providers and receive digital prescriptions directly to their ePA.
The app uses end-to-end encryption to protect users personal health information, and users have full control over who can access their records and for what purposes. There is also the option to cancel the ePA completely.
Prepare an interview study with your primary stakeholders.
Name the stakeholders and explain, why they need to be interviewed. Explain, how you want to contact them.
Justify the type of interview (structured, unstructured, semi-structured).
Prepare the introduction and the closing session as well as the consent form as well as the questions (the interview should be 20 to 30 min long)
Describe how you plan to conduct the interview (Who is taking notes? How do you take notes? Who is asking questions?)
Stakeholders: Health insurance companies in Germany
Reason for interview or email: Health insurance companies are important stakeholders for the Wahl-O-Mat project as they provide healthcare services to the general public. By interviewing health insurance companies, we can gain insights into their ePA policies and practices, which can help the development of the Wahl-O-Mat tool and improve its usefulness for users.
Contact method: We plan to contact health insurance companies via email or webex, requesting a 20-30 minute interview with a representative of the company. We will explain the purpose of the interview and inform them that their responses will be published in our Wahl-O-Mat .
Interview type: Semi-structured interview, as it allows for a flexible conversation while still ensuring that the key topics are covered.
Introduction: We will introduce ourselves, explain the purpose of the interview, and ask for their consent to participate.
Questions:
1. How does your company approach the topic of ePA?
2. How do you ensure the security and privacy of patient data in your ePA systems?
3. Have you or your IT service provider been the victim of a cyber attack in the past?
4. How do you make electronic patient records accessible to patients and healthcare providers?
5. How do you ensure the interoperability of your ePA systems with other healthcare providers?
6. What role do you see ePA playing in the future of healthcare?
7. On what OS versions are your ePA and APP running?
8. Do you have any tutorials on how to install and how to sign in into the ePA?
9. Do you provide a way to use the ePA without a smartphone?
10. Do you provide information about risks on the patients data?
In German (because the communication with the health insurance companies will be in German):
1. Wie wird das Thema ePA in Ihrem Unternehmen angegangen?
2. Wie gewährleisten Sie die Sicherheit und den Datenschutz von Patient*innendaten in Ihren ePA-Systemen?
3. Wurden Sie bzw. Ihr IT-Dienstleister in der Vergangenheit Opfer eines Cyberangriffs?
4. Wie machen Sie elektronische Patientenakten für Patient*innen und Gesundheitsdienstleister*innen zugänglich?
5. Wie stellen Sie die Interoperabilität Ihrer ePA-Systeme mit anderen Gesundheitsdienstleister*innen sicher?
6. Welche Rolle wird die ePA Ihrer Meinung nach zukünftig in der Gesundheitsversorgung spielen?
7. Auf welchen Betriebssystemversionen laufen Ihre ePA und Krankenkassen-App?
8. Stellen Sie Anleitungen für ePA-Registrierungs- und Anmeldungsprozesse zur Verfügung?
9. Bieten Sie eine Möglichkeit, die ePA ohne Smartphone zu nutzen?
10. Informieren Sie über die möglichen Sicherheitsrisiken bzgl. der Patient*innendaten?
Closing session: We will thank the interviewee for their time and input, and ask if they have any additional comments or insights they would like to share.
Consent form: We will use the consent form shown us in the lecture
Unsere Reflexion der letzten Woche:
Wer hat welchen Beitrag geleistet?
Christopher hat sich mit den Fragen befasst und den Ablauf grob geplant. Die anderen haben ergänzt.
Was habt ihr gelernt?
Es ist zeitaufwendig, sich Interviewfragen zu überlegen.
Was lief gut?
Wir haben uns schnell auf unser neues Thema einigen können. Wir hatten unterschiedliche Vorstellungen, welche Stakeholder wir in dem kommenden Interview kontaktieren möchten, die Diskussion darüber war aber sehr konstruktiv, sodass wir nun alle zufrieden mit dem Weg sind, den wir einschlagen wollen.
Was möchtet ihr verbessern?
Und ist nichts aufgefallen, was wir aktuell verbessern möchten